First plant-based coronavirus vaccine shows ‘positive’ results, say GlaxoSmithKline and Medicago
Medicago
said it would file the adjuvanted plant-based coronavirus vaccine for
regulatory approval with Health Canada, the FDA and others.
A 2020 book argues that controlling cancer is within reach if scientists are able to anticipate the evolution of resistance to traditional treatments.
Smithsonian MagazineRead when you’ve got time to spare.

Photo by KATERYNA KON/SCIENCE PHOTO LIBRARY/Getty Images
President Nixon declared the "War on Cancer" with the National Cancer Act of 1971, and in the decades since then cancer researchers have delivered new targeted therapies and immunotherapies that radically improved treatment. Even as more weapons are added to the medical arsenal, however, cancer cells find new ways to resist them.
In a provocative book published in 2020, Athena Aktipis — director of the interdisciplinary cooperation initiative at Arizona State University who studies conflict and cooperation, in a whole range of systems from human societies to cancer cells — argues that humanity may need to rethink our war on cancer by focusing not on eliminating it, but on transforming cancer from a set of deadly, acute diseases to chronic, manageable ones. She writes: "Cancer evolves, but we have the ability to anticipate that evolution and strategically plan our response. We can trick it, send it down a blind alley, sucker it into vulnerability, and shape it into something we can live with."
Aktipis’s book, The Cheating Cell: How Evolution Helps Us Understand and Treat Cancer, came out earlier in the spring and she tells Smithsonian how taking an ecological and evolutionary approach to cancer has led to novel treatment strategies—and why cancer is a lot like the mafia.
What was the impetus for writing this book?
There was a need for a book that would explain the origins of cancer. Why is cancer something that we face as humans, and why do other organisms get cancer? People think cancer is just a modern phenomenon, but it has been around since the beginning of multicellularity. I wanted to tell the story of how evolution operates within our bodies—among our cells over the course of our lifetime—to give rise to cancer.
Cancer treatment traditionally uses high doses of toxic drugs to wipe out cancer cells. But some oncologists have started taking a different approach, inspired by integrated pest management, that seeks to control rather than eliminate. Tell us more about this approach to cancer treatment.
Imagine you have a field and you’re trying to grow crops, but there are pests. If you use high doses of chemical pesticides, then you end up selecting for the pests that can survive despite the pesticide. In cancer treatment, the approach has been to use the highest dose that can be tolerated by the patient.
With integrated pest management, by contrast, you limit the use of pesticides to try to avoid selecting for resistance. You may not get rid of the pests completely, but you can keep their population under control so they do limited harm to the crops. Adaptive cancer therapy is based on the idea that resistance is going to evolve unless we manage the evolution of the resistance itself.
Adaptive therapy is an approach pioneered by Bob Gatenby at Moffitt Cancer Center in Tampa, Florida, who was inspired by integrated pest management approaches. The idea of it is to try to keep the tumor a manageable size and to maintain the ability to treat it with the therapy that's being used. This is very different from hitting it with the highest dose that the patient can tolerate to make it go away, which is the traditional approach. With adaptive therapy, you're just trying to keep the tumor at a stable size and not use so much chemotherapy that you get the evolution of resistance. It is taking a long-term time perspective and thinking about not just what's the immediate effect of the treatment, but what's the long-term effect on the ability to keep the tumor under control.
There are some cancers that we know are curable with high-dose therapy, and so for those, we should continue doing what works. But when it comes to advanced metastatic cancer, that is cancer that has spread from the primary tumor to other organs in the body, it is often the case that you can't eradicate the cancer. You can't achieve a full cure at that point. So it makes sense to change the strategy in those cases to thinking about how the patient can most effectively live with the tumor and how we can keep it from becoming more aggressive. These are important approaches as we truly integrate this evolutionary and ecological cooperation theory for cancer biology.
You call cancer cells “cheaters” because they take advantage of healthy cells without offering any benefit to the body. Why do these harmful cellular cheaters exist across the tree of life?
There's an epic struggle between the way that evolution works on populations of organisms to help suppress cancer and then how evolution works within our bodies. In a population of organisms, the individuals that are the best at resisting cancer are favored. But within an individual body, the cells that are best at replicating and monopolizing resources—and therefore more prone to cancerous behavior—are the ones that are selected. So you have two evolutionary processes in conflict.
A complicating factor is that there can be trade-offs between suppressing cancer and other traits that might enhance your fitness, like having more rapid reproduction and growth. Wound healing is a great example. It is very clear how the same cellular characteristics can both help you heal a wound quickly and lead to susceptibility to cancer. When a wound occurs, the nearby cells need to replicate and migrate to heal the wound. In that environment, the cells in the neighborhood are temporarily more tolerant of cells that replicate and move.
That creates a vulnerability to cancer. You have this possibility that cells will replicate more quickly and move, and that they also create the signaling environment that calls off the immune system. One of the oldest ways to refer to a cancer is actually “the wound that will not heal.”
What tricks have other species evolved to resist cancer that we might be able to use to treat cancer in people?
Cancer is extremely widespread across the tree of life. Some factors seem to predict having more cancer suppression mechanisms. For example, we can think of the cancer suppression gene TP53 as the “cheater detector” of the genome. It is part of this large network that takes in information that could indicate a cell has gone rogue. If the combination of signals is not right, then TP53 triggers a response such as stopping the cell cycle to repair DNA. If that doesn’t work, it triggers cell suicide.
This gene is really important for cancer suppression in a lot of species. Elephants have 22 copies of this gene, while humans only have two. It’s not clear if all the copies in elephants are functional, but elephant cells do have more cell death in response to radiation. The more copies of TP53 your cells have, the more likely they are to undergo programmed cell suicide if they are exposed to a carcinogenic situation. The fact that elephants have more copies of TP53 is an interesting example of how large size can select for having more cancer suppression mechanisms.
In addition to cheating healthy cells, cancer cells cooperate. How can cancer treatments take advantage of this?
Cooperation is not always good. The mafia is an amazing example of cooperation to cheat. There are many parallels in cancer with the way that organized crime uses cooperation within the organization to exploit a broader system. For example, during the 1920s, members of the mafia worked together to take advantage of prohibition and began procuring and selling illegal alcohol. The fortunes that factions made doing this allowed them to dominate organized crime in their cities.
There are several potential approaches involving cell cooperation that we should be exploring more in cancer treatment. Rather than trying to just kill the cancer cells, we can try to disrupt their communication and their adhesion to one another. Those are good targets for intervening in the processes that seem to require cell cooperation, like invasion and metastasis, which are the processes by which cancer cells leave the tumor of origin, circulate in the bloodstream, then invade the tissue of a distant organ. Those invasion events are the seeds of metastases: the spread of cancer throughout the body.
How was it? Save stories you love and never lose them.

team theorised that engineering amyloid into the same hairpin shape before administering it as vaccine

 Professor
Carr added: “While the science is currently still at an early stage, if
these results were to be replicated in human clinical trials, then it
could be transformative"
telegraph.co.uk/news/2021/11/1
Professor
Carr added: “While the science is currently still at an early stage, if
these results were to be replicated in human clinical trials, then it
could be transformative"
telegraph.co.uk/news/2021/11/1 The team theorised that
engineering amyloid into the same hairpin shape before administering it
as vaccine would spur the body into producing antibodies to fight off
that specific structure
telegraph.co.uk/news/2021/11/1
The team theorised that
engineering amyloid into the same hairpin shape before administering it
as vaccine would spur the body into producing antibodies to fight off
that specific structure
telegraph.co.uk/news/2021/11/1

A 'visual prosthesis' implanted directly into the brain has allowed a blind woman to perceive two-dimensional shapes and letters for the first time in 16 years.
The US researchers behind this phenomenal advance in optical prostheses have recently published the results of their experiments, presenting findings that could help revolutionize the way we help those without sight see again.
At age 42, Berna Gomez developed toxic optic neuropathy, a deleterious medical condition that rapidly destroyed the optic nerves connecting her eyes to her brain.
In just a few days, the faces of Gomez' two children and her husband had faded into darkness, and her career as a science teacher had come to an unexpected end.
Then, in 2018, at age 57, Gomez made a brave decision. She volunteered to be the very first person to have a tiny electrode with a hundred microneedles implanted into the visual region of her brain. The prototype would be no larger than a penny, roughly 4 mm by 4 mm, and it would be taken out again after six months.
Unlike retinal implants, which are being explored as means of artificially using light to stimulate the nerves leaving the retina, this particular device, known as the Moran|Cortivis Prosthesis, bypasses the eye and optic nerve completely and goes straight to the source of visual perception.
After undergoing neurosurgery to implant the device in Spain, Gomez spent the next six months going into the lab every day for four hours to undergo tests and training with the new prosthesis.
The first two months were largely spent getting Gomez to differentiate between the spontaneous pinpricks of light she still occasionally sees in her mind, and the spots of light that were induced by direct stimulation of her prosthesis.
Once she could do this, researchers could start presenting her with actual visual challenges.
When an electrode in her prosthesis was stimulated, Gomez reported 'seeing' a prick of light, known as a phosphene. Depending on the strength of the stimulation, the spot of light could be brighter or more faded, a white color or more of a sepia tone.
When more than two electrodes were simultaneously stimulated, Gomez found it easier to perceive the spots of light. Some stimulation patterns looked like closely spaced dots, while others were more like horizontal lines.
"I can see something!" Gomez exclaimed upon glimpsing a white line in her brain in 2018.
Vertical lines were the hardest for researchers to induce, but by the end of training Gomez was able to correctly discriminate between horizontal and vertical patterns with an accuracy of 100 percent.
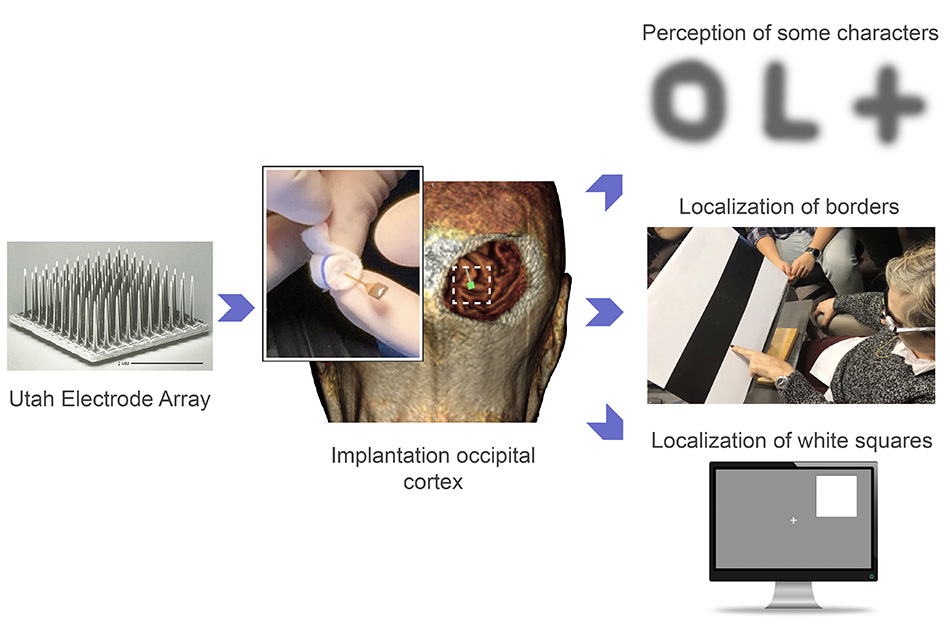 The Utah Electrode Array in action. (John A. Moran Eye Center at the University of Utah)
The Utah Electrode Array in action. (John A. Moran Eye Center at the University of Utah)
"Furthermore, the subject reported that the percepts had more elongated shapes when we increased the distance between the stimulating electrodes," the authors write in their paper.
"This suggests that the phosphene's size and appearance is not only a function of the number of electrodes being stimulated, but also of their spatial distribution… "
Given these promising results, the very last month of the experiment was used to investigate whether Gomez could 'see' letters with her prosthesis.
When up to 16 electrodes were simultaneously stimulated in different patterns, Gomez could reliably identify some letters like I, L, C, V and O. She could even differentiate between an uppercase O and a lowercase o.
The patterns of stimulation needed for the rest of the alphabet are still unknown, but the findings suggest the way we stimulate neurons with electrodes in the brain can create two-dimensional images.
The last part of the experiment involved Gomez wearing special glasses that were embedded with a miniature video camera. This camera scanned objects in front of her and then stimulated different combinations of electrodes in her brain via the prosthesis, thereby creating simple visual images.
The glasses ultimately allowed Gomez to discriminate between the contrasting borders of black and white bars on cardboard. She could even find the location of a large white square on either the left or right half of a computer screen. The more Gomez practiced, the faster she got.
The results are encouraging, but they only exist for a single subject over the course of six months. Before this prototype becomes available for clinical use it will need to be tested among many more patients for much longer periods of time.
Other studies have implanted the same microelectrode arrays, known as Utah Electrode Arrays, into other parts of the brain to help control artificial limbs, so we know they're safe in at least the short term. But it's still early days for the tech, which risks a steady drop in functionality over just a few months of operation.
While engineers beef up the reliability of the devices, we still need to know exactly how to program the software that interprets the visual input.
Last year, researchers at Baylor College of Medicine in Houston inserted a similar device into a deeper part of the visual cortex. Among five study participants, three of whom were sighted and two of whom were blind, the team found the device helped blind people trace the shapes of simple letters like W, S, and Z.
In Gomez's case, there was no evidence of the device triggering neural death, epileptic seizures, or other negative side effects, which is a good sign, and suggests microstimulation can be safely used to restore functional vision, even among those who have suffered irreversible damage to their retinas or optic nerves.
"One goal of this research is to give a blind person more mobility," says bioengineer Richard Normann from the University of Utah.
"It could allow them to identify a person, doorways, or cars easily. It could increase independence and safety. That's what we're working toward."
Right now, it seems only a very rudimentary form of sight can be returned with visual prostheses, but the more we study the brain and these devices among blind and sighted people, the better we will get at figuring out how certain patterns of stimulation can reproduce more complex visual images.
Perhaps one day, other patients in the future will be able to trace the whole alphabet with this prosthesis because of what Gomez has done. Four more patients are already lined up to try out the device.
"I know I am blind, that I will always be blind," Gomez said in a statement a few years ago.
"But I felt like I could do something to help people in the future. I still feel that way."
Gomez's name is listed as co-author on the paper for all her insight and hard work.
The study was published in the Journal of Clinical Investigation.
my suggestion:-
now use ARTIFICIAL INTELLIGENCE TO FIND THE PATTERN OF THE REST OF ALPHABETS,SO THAT
other patients in the
future will be able to trace the whole alphabet

Ata is just six inches tall, with a conical-shaped head and unusually hard bones for her size. Some have claimed that she’s an alien. But a new study published in the journal Genome Research not only continues to disprove the alien theory, but also reveals a scientific explanation for her allegedly extraterrestrial appearance.
The debate started in 2003 when the naturally mummified remains of Ata were discovered near a ghost town in Chile’s Atacama Desert. A Spanish businessman, Ramón Navia-Osorio, purchased the mummy and in 2012 allowed a doctor named Steven Greer to use x-ray and computed tomography (CT) imaging to analyz=se her skeleton.
Greer is the founder of The Disclosure Project, which is “working to fully disclose the facts about UFOs, extraterrestrial intelligence, and classified advanced energy and propulsion systems,” according to its Web site.
Ata is only as long as a human fetus. But a radiologist who analysed the images said that Ata’s bones were about as mature as those of a human six-year-old.
At the time, Greer also provided samples of Ata’s bone marrow to immunologist Garry Nolan at Stanford University in Palo Alto, Calif. Nolan’s team sequenced Ata’s DNA and concluded that her genetic material was from a human being, not an alien. But he couldn’t explain how such a small person could exhibit her unusual physical appearance.

“Once we understood that it was human, the next step was to understand how something could come to look like this,” Nolan says.
So Nolan worked with genetic researchers at Stanford and with computational biologist Atul Butte’s team at the University of California, San Francisco to analyse Ata’s genome. According to their new study, mutations are present in seven of Ata’s genes that are all involved in human growth. Nolan now thinks that this combination of mutations caused Ata’s severe skeletal abnormalities, including her unusually rapid bone growth. He says that Ata is most likely a human fetus who was either stillborn or died soon after birth.
But those who believe that Ata is extraterrestrial aren’t changing their minds, regardless of the new scientific revelations.
“We don’t know what it is, but it most certainly is not a deformed human,” says Greer, who is aware of the new research.
Scientists, however, say that in light of the new analysis, it’s time to bury the Ata controversy.



ZyCoV-D is the first DNA vaccine for people to be approved anywhere in the world.Credit: Zydus Cadila
India has approved a new COVID-19 vaccine that uses circular strands of DNA to prime the immune system against the virus SARS-CoV-2. Researchers have welcomed news of the first DNA vaccine for people to receive approval anywhere in the world, and say many other DNA vaccines might soon be hot on its heels.
ZyCoV-D, which is administered into the skin without an injection, has been found to be 67% protective against symptomatic COVID-19 in clinical trials, and will probably start to be administered in India this month. Although the efficacy is not particularly high compared to that of many other COVID-19 vaccines, the fact that it is a DNA vaccine is significant, say researchers.
It is proof of the principle that DNA vaccines work and can help in controlling the pandemic, says Peter Richmond, a paediatric immunologist at the University of Western Australia in Perth. “This is a really important step forward in the fight to defeat COVID-19 globally, because it demonstrates that we have another class of vaccines that we can use.”
Close to a dozen DNA vaccines against COVID-19 are in clinical trials globally, and at least as many again are in earlier stages of development. DNA vaccines are also being developed for many other diseases.
“If DNA vaccines prove to be successful, this is really the future of vaccinology” because they are easy to manufacture, says Shahid Jameel, a virologist at Ashoka University in Sonipat, India.
The urgency of combating COVID-19 has fast-tracked the development of vaccines that use genetic technology, such as messenger RNA and DNA vaccines, says David Weiner, director of the Vaccine & Immunotherapy Center at the Wistar Institute in Philadelphia, Pennsylvania.
RNA vaccines were quicker to show strong immune responses in clinical trials; they have now been delivered to hundreds of millions of people around the world. But DNA vaccines have a number of benefits, because they are easy to produce and the finished products are more stable than mRNA vaccines, which typically require storage at very low temperatures.
ZyCoV-D was developed by Indian pharmaceutical firm Zydus Cadila, headquartered in Ahmedabad. On 20 August, India’s drug regulator authorized the vaccine for people aged 12 and older. The efficacy figure of 67% came from trials involving more than 28,000 participants, which saw 21 symptomatic cases of COVID-19 in the vaccinated group and 60 among people who received a placebo.
ZyCoV-D contains circular strands of DNA known as plasmids, which encode the spike protein of SARS-CoV-2, together with a promoter sequence for turning the gene on. Once the plasmids enter the nuclei of cells, they are converted into mRNA, which travels to the main body of the cell, the cytoplasm, and is translated into the spike protein itself. The body’s immune system then mounts a response against the protein, and produces tailored immune cells that can clear future infections. Plasmids typically degrade within weeks to months, but the immunity remains.
Both DNA and mRNA vaccines have been under development since the 1990s, says Weiner. The challenge for DNA vaccines is that they need to make it all the way to the cell nucleus, unlike mRNA vaccines, which just need to get to the cytoplasm, says Jameel. So, for a long time, DNA vaccines struggled to induce potent immune responses in clinical trials, which is why they had been approved for use as vaccines only in animals, such as horses, until now.
To solve this problem, ZyCoV-D is deposited under the skin, as opposed to deep in muscle tissue. The area under the skin is rich in immune cells that gobble up foreign objects, such as vaccine particles, and process them. “This helps capture the DNA far more efficiently than in the muscle,” Jameel says. Unusually, the vaccine is delivered using a needle-free device pressed against the skin, which creates a fine, high-pressure stream of fluid that punctures the surface and is less painful than an injection.
But despite being more potent than previous DNA vaccines, ZyCoV-D requires a minimum of three doses to achieve its initial efficacy. This is likely to add to the logistical challenge of administering the vaccine during the current pandemic, says Jameel.
Although ZyCoV-D’s efficacy seems to be lower than the 90% or higher achieved by some mRNA vaccines, the figures are not comparable, says Jameel. The ZyCoV-D trials in India earlier this year were conducted while the Delta variant of SARS-CoV-2 was the dominant variant in circulation, whereas earlier mRNA vaccine trials were conducted when less transmissible variants were circulating. “The efficacy is essentially against the Delta variant, so that is pretty good,” he says.
Some researchers have criticized a lack of transparency in the approval process, because no late-stage trial results have yet been published. Zydus Cadila says the trial is still under way and it will submit the full analysis for publication shortly. The company says the first doses will start to be administered in India in September and it plans to produce up to 50 million doses by early next year.
Many DNA vaccines against COVID-19 are currently undergoing clinical trials around the world.
Vaccine |
Developer |
Location |
Route |
Stage of trial |
ZyCoV-D |
Zydus Cadila |
India |
Skin |
Approved for emergency use |
INO-4800 |
Inovio and partners |
United States |
Skin |
Phase II/III |
AG0302-COVID19 |
AnGes, Osaka University, Takara Bio |
Japan |
Muscle |
Phase II/III |
GX-19N |
Genexine |
South Korea |
Muscle |
Phase I/II |
GLS-5310 |
GeneOne Life Science |
South Korea |
Skin |
Phase I/II |
COVID-eVax |
Takis, Rottapharm Biotech |
Italy |
Muscle |
Phase I/II |
AG0301-COVID19 |
AnGes, OSaka University, Takara Bio |
Japan |
Muscle |
Phase I/II |
Covigenix VAX-001 |
Entos Pharmaceuticals |
Canada |
Muscle |
Phase I |
CORVax12 |
OncoSec, Providence Cancer Institute |
United States |
Skin |
Phase I |
bacTRL-Spike |
Symvivo |
Canada |
Oral |
Phase I |
COVIGEN |
BioNet, Technovalia, University of Sydney |
Thailand, Australia |
Skin or muscle |
Phase I |
Several other DNA vaccines are being developed against COVID-19, using a variety of antigens and delivery mechanisms (see ‘DNA vaccines in clinical trials’). Two have entered late-stage trials: one by Japanese company AnGes, based in Osaka; the other, which Weiner helped to develop, by Inovio Pharmaceuticals in Plymouth Meeting, Pennsylvania. Inovio is injected under the skin and uses a device that hits the skin with short electric pulses to form pores in the cells that the vaccine can slip through.
More than half a dozen DNA vaccines for COVID-19 are in early-stage trials, including one by the South Korean biotech company GeneOne Life Science in Seoul, and another that Richmond is involved in, developed by the Thai firm BioNet in Bangkok. This vaccine is undergoing a phase I trial in Australia.
But Richmond expects many more DNA vaccines to emerge, targeting diseases for which there are currently no vaccines — from cytomegalovirus, which can be passed on to babies during pregnancy, to respiratory syncytial virus. DNA vaccines are also being trialled or developed for influenza, human papillomavirus, HIV and Zika.
DNA vaccines can store lots of information, which means they can encode large, complex proteins or even multiple proteins. Weiner says that gives them promise as anti-cancer vaccines, a possibility he is exploring in his own research.
“It’s a very exciting time for genetic technologies. They have finally gotten a chance to show what they can do,” he says.
Nature 597, 161-162 (2021)
doi: https://doi.org/10.1038/d41586-021-02385-x

