8 days ago — Known as 'IHU', the B.1.640.2 variant has been reported by researchers at institute IHU Mediterranee Infection in at least 12 cases, and has ...
04-Jan-2022 — Known as 'IHU', the B.1.640.2 variant has been reported by researchers at institute IHU Mediterranee Infection in at least 12 cases, and has ...
8 days ago — Known as 'IHU', the B.1.640.2 variant has been reported by researchers at institute IHU Mediterranee Infection in at least 12 cases, and has ...
04-Jan-2022 — Known as 'IHU', the B.1.640.2 variant has been reported by researchers at institute IHU Mediterranee Infection in at least 12 cases, and has ...
16-Dec-2018 — At Sonapur, 20 km from Guwahati, Dr Dhani Ram Baruah sits in his ... two decades after being arrested for transplanting a pig heart to a ..
US doctors transplant full, live pig heart into human patient
In
this photo provided by the University of Maryland School of Medicine,
members of the surgical team show the pig heart for transplant into
patient David Bennett in Baltimore on Friday. (AP)
WASHINGTON:
Whether or not pigs have wings or pigs can fly, pigs can certainly save
human lives. In a landmark first-of-its kind surgery, doctors at the
University of Maryland School of Medicine outside Washington DC have
successfully transplanted a genetically modified pig heart into a
57-year-patient with terminal illness. The patient, Maryland resident David Bennett,
is doing well three days after the surgery, the university's medical
center said on Monday, as doctors who performed the operation revealed
the transplanted heart was working normally and creating the pulse and
pressure associated with the human heart. The surgery took place on
Friday and took about eight hours.
Video Player is loading.
Although
the patient is still connected to a heart-lung bypass machine which was
keeping him alive before the operation, doctors said the new heart is
doing most of the work and there are no signs of rejection as of now. He
is expected to be taken off the machine on Tuesday. "We are
proceeding cautiously, but we are also optimistic that this
first-in-the-world surgery will provide an important new option for
patients in the future," Dr Bartley P. Griffith, the lead surgeon in the breakthrough achievement said, while foreseeing a solution to organ shortage crisis in the long run. While
some pig organs and cells, notably its heart valve and skin, have been
used in humans before, this is the first time a full porcine heart has
been transplanted into a human. The pioneer in this field of
transplanting animal organs -- called xenotransplantation -- is
Pakistani-American Dr Mohammed Mohiuddin,
a graduate of Karachi's Dow Medical College, who with Dr Griffith set
up UMSOM's Cardiac Xenotransplantation Program and was part of the
surgery team. "This is the culmination of years of highly
complicated research to hone this technique in animals with survival
times that have reached beyond nine months. The FDA used our data and
data on the experimental pig to authorize the transplant in an end-stage
heart disease patient who had no other treatment options," Dr.
Mohiuddin said, adding that the successful procedure provided valuable
information to improve the potentially life-saving method in future
patients. Doctors had to go in for a porcine heart transplant rather
than a conventional one because Bennett's condition did not allow him
to qualify for a human transplant. He had been admitted to the hospital
more than six weeks earlier with life-threatening arrythmia and was
connected to a heart-lung bypass machine, called extracorporeal membrane
oxygenation (ECMO), to remain alive, the university said. In addition
to not qualifying to be on the transplant list, he was also deemed
ineligible for an artificial heart pump due to his arrhythmia. He
then consented to a porcine transplant even after being told of the
risks. “It was either die or do this transplant. I want to live. I know
it’s a shot in the dark, but it’s my last choice,” he said the day
before the surgery. According to Dr Griffith, when briefed about the
unprecedented nature of the procedure, Bennett joked, "Well, will I
oink?" Bennett won praise from doctors and administrators for his do
or die decision. "We appreciate the tremendous courage of this live
recipient, who has made an extraordinary decision to participate in this
groundbreaking procedure to not only potentially extend his own life,
but also for the future benefit of others," Dr Mohan Suntha, President and CEO of the University of Maryland Medical System said.
It
is time to remember Dr Dhaniram Baruah for doing the same was arrested.
Instead of accolades, Indian scientists are named and shamed. Dr Subhas
Mukhopadhyay who paid the price with his life was a pioneering example.
16-Dec-2018 — At Sonapur, 20 km from Guwahati, Dr Dhani Ram Baruah sits in his ... two decades after being arrested for transplanting a pig heart to a ...
===========================================
Pig heart transplant: Not many are buying the Assam doctor's story yet
Not many are buying the Assam doctor's story yet.
advertisement
RUBEN BANERJEE
Guwahati January 15, 1997
ISSUE DATE: January 15, 1997
UPDATED: April 16, 2013 11:54 IST
In
the sterile and sombre air of an intensive care unit, Purna Saikia
fights for life. A machine helps him breathe; tubes and pipes snake
around and into him. Nothing unusual except the failing heart inside
Saikia is a pig's.
Or so Dr Dhani Ram Baruah says. "Medical
science has taken a giant leap forward," exults Baruah, the head of the
Dhani Ram Baruah Heart Institute outside Guwahati. Few share Baruah's
excitement. Xenotransplantation, or animal-to-human transplant, has
never worked on the heart.
No one has yet figured out how to stop the
human body's immune system from waging a war against animal hearts, a
process called rejection.
While researchers explore the molecular
world for clues to stop the immune system, Baruah has a simple solution
literally. It's a secret solution of chemicals that blinds the immune
system, he says. Saikia's heart was treated with the magic solution for
30 minutes, washed and then implanted in a 15-hour operation, Baruah
explains.
So does a pig's heart beat in the dying Saikia? "It's a
hoax... cheap publicity," fumes Assam's Health Minister Dr Kamala
Kalita. "No pig's heart was implanted in the first place." Indeed Baruah
signed a statement saying he had done no transplant, but he alleges the
confession was forced from him. "They threatened to shut down my
hospital if I did not comply."
"If the present heart shows signs of failing I will have another pig heart implanted." Dr Dhani Ram Baruah
Unfortunately,
no one in the medical fraternity believes him either. "It sounds like
something out of a dream," laughs N.K. Mehra, head, department of
histocompatibility and immunogenetics, All India Institute of Medical
Sciences, New Delhi. If something fools the immune system, the diverse
triggering mechanisms somehow find a way around.
"I would be
very, very sceptical," says William Baldwin, a xenotransplantation
researcher at John Hopkins University in the US, where one of the
world's top teams hasn't got beyond getting pig's hearts into baboons.
And these are pigs genetically engineered to reduce rejection; Dr
Baruah's pigs are your ordinary porkers. Experiments on human beings
stopped after Baby Fae, a two-week-old baby in the US, died within three
weeks in 1984 after her heart was replaced with a baboon's heart.
Little
wonder then, that Dr Baruah is being termed the medical fraternity's
Ramar Pillai, the man who held a nation in thrall last year when he
claimed to make fuel from water. But Dr Baruah is no small-town hick.
He's a Fellow of the Royal College of Surgeons in the UK, and was joined
in the operation by Dr Jonathan Ho, a cardiac surgeon from the Prince
of Wales Hospital in Hong Kong.
Saikia in intensive care: the transplant has led to questions of medical ethics
But
INDIA TODAY has learned that Drs Baruah and Ho have achieved infamy in
the past. They implanted heart valves made of animal tissue - developed
by Dr Baruah in 12 patients in Hong Kong in 1992. A year later, six
patients died. The Asian Medical News reported that "grave concerns"
were expressed "over the procedure and ethics of the implementation".
Ethics
raise their inconvenient head again. The most pointed question about
xenotransplantation may not be whether it can be done but whether it
should be done. Deadly new viruses could spread to humans from animals,
much as AIDS moved from monkeys. "This is totally against the ethics of
medical science," says Mehra.
The good doctor is undaunted. "To
hell with controversies," he says angrily. "I will go ahead with what I
am supposed to do." Back in the intensive care ward, Saikia is in
critical condition. What if he dies? Baruah doesn't blink: "If his
present heart shows signs of failing, I will have another pig heart
implanted." Simple.
7 days ago — Scientist Dr. Peter Scott-Morgan is pushing the boundaries of what it means to be human. Dr. Peter Scott Morgan, scientist and cyborg. Channel 4.
New frontiers
After ALS struck, he became the world’s most advanced cyborg
Scientist Dr. Peter Scott-Morgan is pushing the boundaries of what it means to be human.
Dr.
Peter Scott-Morgan, a prominent British-American robotics scientist, is
almost completely paralyzed — save for his piercing blue-gray eyes,
which are constantly in motion, typing out text to be spoken by his
synthesized voice.
Scott-Morgan, who is 63, remains undaunted,
though. “Paralysis is an engineering problem,” he insists, and it’s one
he has a solution for: becoming a cyborg. “And when I say ‘cyborg,’ I
don’t just mean any old cyborg, you understand, but by far the most
advanced human cybernetic organism ever created in 13.8 billion years,”
he says.
In 2017, Scott-Morgan was diagnosed with amyotrophic lateral sclerosis (ALS),
also known as Lou Gehrig’s disease. His illness, called Motor Neurone
Disease (MND) in Britain, is the same degenerative disease that
afflicted physicist Stephen Hawking. Having spent equal periods of his
career living in England and America, he now resides in Torquay, a
seaside town in southwest England, with his husband Francis.
He’s been well-known in the U.K. since the 2020 release of a primetime Channel 4 documentary, Peter: The Human Cyborg, and his subsequent memoir, Peter 2.0. Here in the U.S., he is a more obscure figure.
ALS
affects the motor neurons in the brain and spinal cord that tell
muscles what to do. As ALS progresses, the degeneration of motor neurons
in the brain interferes with messages to muscles in the body.
Eventually, muscles atrophy, and people with ALS lose the ability to
move their arms, legs, and body. They become unable to talk, walk,
breathe, or swallow. Most die from respiratory failure within three to five years after symptoms first appear.
In
2017, doctors told Scott-Morgan that he had two years to live. So far,
it’s been four — and he has no intention of dying anytime soon. Dr.
Brian Dickie, director of research for the MND Association in the U.K.,
who is familiar with Scott-Morgan’s case, says the roboticist has what
those in the terminal-disease world call “incurable optimism.”
Scott-Morgan doesn’t believe in God; he believes that technology will save him. “All my early science education came from Dr. Who and Star Trek,” he says. “They taught me that if you’re smart enough, brave enough, and have access to technology, anything’s possible.”
At
this point, Scott-Morgan is almost completely “locked-in,” unable to
move except for his eyes and a few facial muscles. His sense of smell
and taste are gone, and he can’t breathe on his own, but his brilliant
mind is fully intact.
Scott-Morgan now relies on a synthetic version of his biological voice and has had his face scanned to produce a 3D animated avatar,
which he wears on a screen on his chest when speaking publicly. After a
series of operations to extend his life, including a total
laryngectomy, he uses technologies like GPT-2, OpenAI’s generative deep-learning model for text, pushing the boundaries of what it means to be human.
He’s done all this with a global consortium of technologists, designers, and physicians. The Rebels, he calls them. His Scott-Morgan Foundation
is collaborating with companies like Intel, CereProc, DXC, and Lenovo.
They are working alongside leading scientists, engineers, artists, and
technologists to provide hardware, software support, integration, and
AI. They’re all donating their time and resources in an effort to
pioneer better solutions for people living with extreme disabilities.
Exclusive video of Scott-Morgan speaking via his old and new avatarsPeter Scott-Morgan
The
Rebels are working on advancing the ability to customize expressive
digital voices, developing self-driving wheelchairs, and embedding smart
technology throughout Scott-Morgan’s home.
“With extraordinary
support from my husband, Francis, and countless kind and brilliant
collaborators, I find the once-dark future incredibly bright,” says
Scott-Morgan, whose ultimate goal is to control his synthetic voice,
avatar, word predictor, self-driving vehicle, and exoskeleton through a
single user interface. To do so, he plans to increasingly rely on AI.
“Cyborg
is just a fancy word for part-human, part-machine,” he says. “Contrary
to the torturous scare stories about how it feels to be trapped in your
own living corpse, the brain moves on. It grieves a bit, and then, if
you give it a chance, most of the time, it forgets. Days pass when I
never once remember that I could walk, move, or absurdly, even that I
could talk in the past.”
Scott-Morgan says he participated in the
recent documentary about him to get a message of “thriving” out there to
counter our culture’s defeatism around terminal illness. “Society just
expects people like me to statistically curl up and die on cue,” says
Scott-Morgan. “Instead,I intend to be a human guinea pig, to see just how far we can turn science fiction into reality.”
Locked-in
The
first time I hear from Scott-Morgan, in July, he emails me a 111-page
PowerPoint presentation for his foundation, which took him a month to
complete using only his eyes. “Some days, I could only design two slides
a day,” he writes.
One of Scott-Morgan’s slides describes a night
when he couldn’t communicate an excruciating pain from a cramp in his
foot. (Between 57 and 72 percent of patients with ALS report pain.)
Not
long after, I wake up with a cramp in my own foot. At first, I think
I’m having a nightmare, psychosomatically channeling Scott-Morgan’s
pain. I can’t conceptualize the feeling of being locked-in and
experiencing unmanageable suffering. For seconds, which feel like
minutes, I try to calm my mind. I can't think my way out of the cramp, a
fact that takes me a while to shake. If I couldn't manage the pain, how
does Scott-Morgan?
The following morning, I email Scott-Morgan
about my experience, worried about what it must be like for him. “To put
this in perspective, temporarily losing the ability to use a hi-tech
comms system — although potentially traumatic and painful — is
infinitely preferable to not having the system at all and suffering the
waking nightmare of being locked-in, trapped in impotent silence within
the straightjacket of your own living corpse,” he responds.
“Fortunately,
there is a well-established protocol for high tech,” he adds. He
suggests I talk to Lenovo’s chief technology officer, Thorsten Stremlau.
“There are rare moments where you see the real power and potential of technology, where the possibilities both seem endless and essential.”
Lenovo
is providing the intelligent hardware — smart cameras, eye-tracking
headsets, and high-performance computing infrastructure — needed to
realize Scott-Morgan's vision. “There are rare moments where you see the
real power and potential of technology, where the possibilities both
seem endless and essential,” says Stremlau when we connect via Zoom.
“Meeting Dr. Peter Scott-Morgan was one of those moments.”
One
of the earliest project teams Stremlau was part of at Lenovo aided
Stephen Hawking with the IT setup for his wheelchair and laptop.
Expanding on that work, Stremlau plans to use cameras and wearables to
detect distress or elevated vitals in Scott-Morgan; the tech will alert
his caretakers should he be unable to communicate because he’s not
wearing a headset.
“These problems we solve for Scott-Morgan will help us advance the work we’re doing for people facing disabilities,” Stremlau says. “Ensuring that Peter has a way to communicate when he’s locked-in drives my commitment.”
Triple-ostomy
As
a 16-year-old growing up in Wimbledon, England, Scott-Morgan wrote
essays about how in the future, his human brain would link with an
electronic brain, asserting that “together we will be far more
intelligent than the sum of our parts.”
In 1984, he published The Robotics Revolution,
a book about the future of robots, almost as if he knew he’d need a
manual. Building on a bachelor’s degree in computing science, and a
post-graduate diploma in AI, he earned a Ph.D. in robotics from the
Imperial College of Science, Technology, and Medicine — the first such
degree granted in England.
When
Scott-Morgan came out as gay in the 1970s, everyone in his family,
except his parents, disowned him. “The world told me, ‘You really don’t
fit,’” he says. When the Citizen Partnership Act was enacted in the U.K.
in 2005, Scott-Morgan and his partner, Francis, became the country’s
first legally recognized homosexual couple. After the law was revised in
2014, the two were the first to officially marry there.
The Scott-Morgans at their weddingPeter Scott-Morgan
In
2017, just after being diagnosed with ALS, Scott-Morgan realized he’d
need to act quickly to reengineer his body before becoming locked-in. He
envisioned three surgeries: a gastrostomy, colostomy, and a cystostomy,
which would insert tubes directly into his stomach, colon, and bladder,
respectively. A “triple-ostomy” he called it. The surgeries would allow
Scott-Morgan to take in more nutrients and avoid having to have a
full-time caretaker to assist him in going to the bathroom.
The
challenge was that no one with ALS had ever preemptively had all three
surgeries, let alone requested them. Determined, Scott-Morgan and his
husband met with the head of the ALS clinic at a major London teaching
hospital to describe his plan. However, as Scott-Morgan recounts in his
book, before he finished explaining his reasoning, the doctor
interrupted him: “I refuse to become involved in any of this!”
“But I want to be proactive in my overall clinical care,” said Scott-Morgan.
“ALS
follows no rules. You cannot be anything other than reactive,” said the
doctor. “Plus, if we did that for you, we’d have to do it for everyone
with ALS.”
Scott-Morgan processed this and sat in disbelief. Imaginerejecting individualized care, he thought. He fired the doctor and returned home to meet with his local National Health Service physicians doctors.
When
Scott-Morgan explained the “triple-ostomy” to Tracy Thomas, his local
ALS coordinator, she did not take well to the idea. “When I said I was
going to throw a huge amount of cutting-edge technology at my disease to
see how I can make being locked-in really exciting,” says Scott-Morgan,
“she let me know that it would be a newly frozen hell before any
surgeon on the planet would damage perfectly healthy organs.”
The
plan was radical, and to further complicate the situation, most doctors
are hesitant to operate on a patient with ALS because general
anesthesia can impede breathing. Also, some physicians worry that
surgery may trigger a more rapid progression of their disease.
Ultimately,
Thomas was won over by Scott-Morgan’s enthusiasm to extend his life and
organized a meeting with Dr. Maree Wright, a soft-spoken
anesthesiologist based in his hometown. “When I first heard about
Peter’s case, I thought, ‘Why would he want this really high-risk
surgery?’ But you know,” says Wright via Zoom, “there’s only one Peter.”
She lifts her hands and smiles. “He’s a trailblazer, and frankly, we
need people that rock the boat to make us think and reflect on why we do
things in a certain way.”
Wright was caught off guard by the
passion and candor with which Scott-Morgan expressed his desire to live.
It shook her views on how the medical profession approached the
treatment of his disease. If she could help him, the implications for
other ALS patients could be staggering.
However,
first, she had to develop an anesthesia plan, and there was hardly any
research data on how to anesthetize people with ALS. Her greatest
concern was that Scott-Morgan might not be able to come off a ventilator
after his operation. Hospital officials tried to talk Scott-Morgan out
of having his surgery at the eleventh hour, but he was resolute in his
decision to move forward.
Ultimately, Scott-Morgan’s team of
physicians and his local NHS hospital made the bold decision to support
his wishes and move forward with the landmark surgeries that would
extend his life. On July 10, 2018, the three surgeries were performed by
multiple surgeons over three hours and 40 minutes.
Everyone
involved was surprised to see Scott-Morgan discharged to the general
surgical ward after only a day in ICU and then sent home 15 days
post-op. Scott-Morgan proudly points out that a medical paper about the procedure was selected as the Oxford Medical Case Report of the year for 2019.
Version 2.0
Immediately
after his triple-ostomy, Scott-Morgan began planning his next surgery, a
full laryngectomy to stop the risk of choking on his own saliva or not
getting enough oxygen. It was another radical idea — one that would cost
Scott-Morgan his voice box but prolong his life indefinitely.
Wright,
Scott-Morgan’s anesthesiologist, helped him find the surgeon to do it:
Dr. Philip Reece, a top ear, nose, and throat surgeon also based locally
in Devon. Reece agreed with Wright that Scott-Morgan should be able to
live as full a life as possible.
Before the surgery happened,
Scott-Morgan set out to solve another problem — how to create a
synthetic voice that sounded like him. He reached out to a world
authority in speech technology research and development, Dr. Matthew
Aylett, the chief scientific officer of CereProc, a company that creates
text-to-speech solutions. Based in Edinburgh, Scotland, CereProc is the
company that rebuilt film critic Roger Ebert’s voice following his throat cancer surgery.
“Because of new translation technologies, I will be able to swear in any language.”
Using a neural text-to-speech system called CereWave AI,
Dr. Aylett created a digital voice that sounds very close to
Scott-Morgan’s natural voice. CereProc reproduces emotion by asking
speakers to read scripts in different ways — say in a calm or tense
tone.
“If
you lose your voice because of an illness like ALS, you want to sound
like you,” says Aylett. “Synthetic-voice technology is evolving daily.
From changes in algorithms to improvements in how we process and edit
voice itself, it is becoming quicker, easier, and more efficient to
create an artificial voice.”
As Scott-Morgan’s ALS progresses, he
won’t be unable to form facial expressions, so he wanted a 3D animated
avatar that could express emotions and be capable of speech. Aylett’s
team worked with Scott-Morgan to record more than 15 hours of audio and
more than 1,000 individual phrases to create the avatar.
On Oct. 9, 2019, Scott-Morgan tweeted what he said was his last post as “Peter 1.0.”
The
following day, he struggled to say his last words to his partner — “I
love you” — just before Reece performed the landmark preemptive
procedure, the first-ever elective laryngectomy on someone with ALS in
the U.K.
“Being
able to speak with what is recognizably my voice, has totally taken the
sting out of giving up my biological voice,” says Scott-Morgan.“Because
of new translation technologies, I will be able to swear in any
language,” he adds. “Shit! Merde! Scheisse!” His digital avatar can even
sing, as demonstrated in a recent live interview with broadcaster
Stephen Fry.
Scott-Morgan’s first-generation avatar couldn’t smile. His new AI-instructed avatar — created by Pinewood Studios, which digitally duplicated Carrie Fisher’s face for the latest Star Wars
movie — will show his emotions, allowing him to laugh, smile, wink, and
pull off his signature move: raising his right eyebrow. Currently, the
challenge is real-time synchronization — so voice, lips, and expressions
all work together to portray the same emotion — something we take for
granted as human beings.
“My smile will be the last thing to
disappear,” says Scott-Morgan. “I should have a new avatar just in time
before I can no longer smile. They promise it will be indistinguishable
from a real person, allowing me to convey emotion.”
AI system
Today
Scott-Morgan is limited to communicating letter by letter, word by
word, through a manual eye-tracking system. DXC is working with the
Scott-Morgan Foundation and partners to develop a new context-aware AI
system that will radically improve the verbal spontaneity of Peter 2.0.
The
next iteration of the software will include a system that will learn
from Peter’s previous interactions and offer him possible responses
appropriate to his situation. (Before being locked-in, Scott-Morgan had
laser eye surgery to give him perfect vision at 70 centimeters — the
distance from eyes to his computer screen.)
Esther Duran, design and innovation director at the Scott-Morgan Foundation, collaborated with Lama Nachman,
director of the Human & AI Systems Research Lab at Intel, to help
Scott-Morgan communicate. Previously, Nachman and her team developed
Intel’s Assistive Context-Aware Toolkit,
a software platform that helped Hawking communicate through keyboard
simulation, word prediction, and speech synthesis. They made it
open-source so that developers could build different capabilities on top
of it.
“I prefer to view the future through the lens of human–AI collaboration rather than human–AI competition.”
After
Hawking lost the use of his hands, he started using a cheek muscle to
communicate. Computers designed for him relied on running lists of
words. Whenever the cursor reached a word or phrase he wished to use,
Hawking twitched his cheek muscle to select it. The process was
painstakingly slow — about one word per minute.
Nachman explains
that extreme accuracy mattered to Hawking, so he wasn’t willing to give
up control. “Whereas, if you look at Peter, he wants to have a natural
interaction with people,” she says. “It’s not about wanting to sound
exactly like Peter 1.0 before his diagnosis. He’s trying to meld with
his AI to make Peter 2.0 the best combination of his personality and the
AI.
“While
much of the conversation around AI and humans positions the
relationship between the two as adversarial,” she continues, “I prefer
to view the future through the lens of human–AI collaboration rather
than human–AI competition.”
The future
The
next challenge the Rebels are tackling is motion, and they are
recreating every element of both the mental and mobile human experience.
DXC is helping to integrate Scott-Morgan’s AI to control his
specialized robotic wheelchair, a sophisticated device that can “boldly go where no wheelchair has gone before,” as Morgan put it in a tweet.
“The
development of self-driving wheelchairs has some clear first-mover
advantages over cars,” says Sukhi Gill, DXC’s chief technology officer
for Europe, Middle East, and Africa. “They operate mostly in known and
controlled environments — think home, garden, park, and local store.
They move a lot slower and have to contend with far fewer possible
hazards. By applying some learnings and technologies from the automotive
industry, the self-driving wheelchair represents a realistic mid-term
goal for this project.”
Ever
the optimist, Scott-Morgan says he envisions “being able to speed
through an obstacle course or safely make my way through a showroom of
porcelain vases.”
Meanwhile, says Jerry Overton, vice chair and
director of AI at the Scott-Morgan Foundation, there’s an ongoing
project to give Scott-Morgan the smartest home possible. “We are
designing Peter's home as a network of home-automation devices and
personal applications.”
This network includes smart thermostats,
smart bulbs, motion sensors, cameras, his avatar, and messaging
applications. “Finally, we are using a central artificial intelligence —
nicknamed CHARLIE — to coordinate the network,” he adds. Overton offers
an example of what would happen if Scott-Morgan's biosensors suggest
that his body temperature is becoming too high: “CHARLIE can take the
initiative to lower the room temperature and alert his healthcare
providers that there may be a problem.”
It takes a rare person to
serve as a living tech experiment. As I got to know Scott-Morgan, I
continually asked myself if I could ever endure the exceedingly
uncertain nature and psychologically harrowing experience of rewiring my
entire persona.
I didn’t know. So I asked the person closest to
Scott-Morgan what he thinks. “As things are today, I might not wish to
stay alive as long as Peter has if I were to get ALS,” says his husband,
Francis. “But I hope that if you ask me again in five years that my
answer will absolutely be yes.”
The
following day, I receive an email from Scott-Morgan, who has obviously
heard about my question to Francis. The subject line reads “Love never
dies.” “Whatever Francis tells you (and tells himself) about not being
as brave as me, that is what is scientifically categorized as
‘bollocks’!” he writes. “Bravery isn’t about not feeling scared, it’s
feeling scared but going on regardless.
The Scott-Morgans in the early 1980sPeter Scott-Morgan
The Scott-Morgans in 2020Peter Scott-Morgan
“Here’s
how it would play out,” he continues. “If Francis ever felt like giving
up, I would remind him (as he occasionally does to me) that that’s not
what Scott-Morgans do. ALS is the ultimate bully, and we have never
given in to bullies. I would reassure him that I would always be there,
fighting by his side.”
The most extraordinary thing about
Scott-Morgan, beyond his defiant optimism, is that he sees his diagnosis
as a blessing, not a curse. “Without my ALS, Francis and I would have
enjoyed ourselves but achieved little,” he says. “Now we may be able to
help rewrite the future of what it means to be disabled. How do you
weigh a trade-off as gargantuan as that?”
I
realize that I’ve never known anyone so adamantly alive. His closing
words speak to what inspires all the Rebels. “Ultimately, however
uncertain Francis may feel now, I am not in the least uncertain — for
one very simple reason,” writes Scott-Morgan. “If there is one thing
that is certain in my universe, Francis would never voluntarily leave me
alone. Any more than I would him.
“I am a prime candidate for the
fast track to death, but I will pass on the offer,” he adds. “I am
frankly far too busy having fun.”
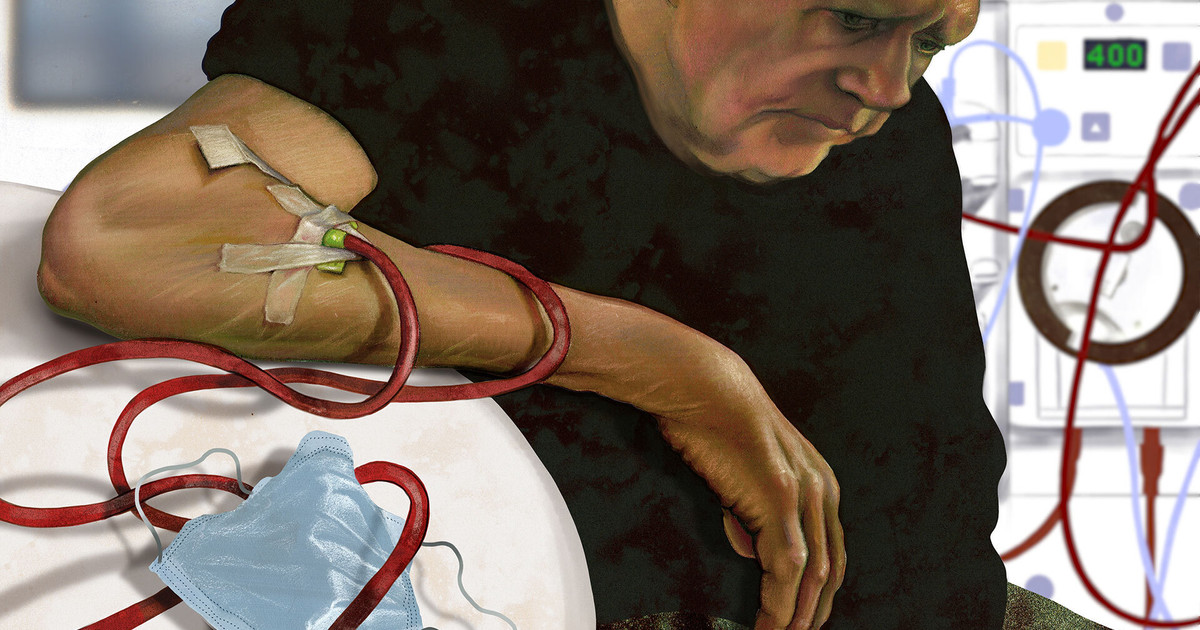
8 days ago — The pandemic killed so many dialysis patients that their total number shrunk for the first time in nearly half a century. Few people took ...
Republish our articles for free, online or in print, under Creative Commons licence.
The western world has written plenty about its high-profile COVID
vaccines: the mRNA products of Pfizer and Moderna, viral-vectored jabs
from AstraZeneca and Johnson & Johnson, and those that are just
emerging, such as Novavax’s protein-based vaccine. Many countries are relying on them for protection.
But not Cuba. It’s been quietly working on its own vaccines, immunising its population and selling doses abroad.
Cuba’s vaccine efforts have maintained a relatively low profile in
the west to date. Politics may well be a reason. The US embargo against
Cuba that began in the cold war is still in effect, and tensions between the countries remain high.
But for those familiar with Cuba, its COVID vaccine development should come as no surprise – the country has a long history
of manufacturing its own vaccines and medicines. Nor should it be
surprising that two of its COVID vaccines – Abdala and Soberana 02 –
appear to have performed very well in trials. Here’s how they work.
Abdala is a protein subunit vaccine, which is a well-established design. The hepatitis B vaccine and Novavax COVID vaccine
use this approach. These vaccines work by delivering just a portion of
the virus that they’re targeted against – in the case of Abdala, bits of
the coronavirus’s spike proteins, which cover its exterior.
The proteins used in the vaccine aren’t taken from the coronavirus directly. Instead, they’re grown in cells of a yeast (Pichia pastoris) that have been specially engineered.
Cuba has long punched above its weight when it comes to healthcare and biotechnology.Ernesto Mastrascusa/EPA-EFE
On their own, the portions of spike protein are harmless. But when
the immune system encounters them, it still trains itself to recognise
and destroy them. If the full coronavirus is then encountered in the
future, the body will attack these outer parts of the virus and quickly
destroy it. Abdala is given in three doses.
The other Cuban COVID vaccine, Soberana 02, uses a “conjugate”
design, along the lines of meningitis or typhoid vaccines. It contains a
different part of the spike protein to Abdala and generates an immune
response by attaching (conjugating) this to a harmless extract from the
tetanus toxin. When the body encounters these linked together, it
launches a stronger immune response than it would to either alone.
Soberana 02 is produced in hamster ovary cells, a process that can be slow, and this may restrict large-scale manufacturing.
Originally, it was given as two doses, but researchers later
identified that a third dose would be beneficial. This booster dose
contains just the spike protein parts, without the tetanus toxin, and is
known as “Soberana Plus”.
How effective are they?
Both vaccines have been approved by the Cuban regulator, though they started being rolled out in May – before authorisation had been granted – in response to a rise in cases. There have been concerns about a lack of information on their safety and efficacy.
On November 1 2021, a preprint
(research still awaiting review) was finally published of a Soberana
phase 3 trial that included 44,031 participants. The results suggest
that two doses of Soberana 02 with a booster of Soberana Plus are
together 92% protective against symptomatic COVID. The preprint notes
that during the trial, the vaccine was most likely being tested against beta or delta – two variants of the coronavirus that other vaccines have found harder to control.
Before this, a phase 1 study
of giving Soberana Plus to people who had already had COVID was
published in September. This was testing the effects of Soberana Plus as
a booster to natural rather than vaccine-induced immunity. It showed no
safety issues and stimulated a good immune response when used in this
way – though the study was small, involving just 30 participants.
For Abdala, the only phase 3 trial data available was issued by Cuban press releases in June and July
2021. The three-dose schedule is also reportedly 92% protective against
symptomatic COVID as well as allegedly fully protective against severe
disease and death.
This generated huge enthusiasm within Cuba. However, since then little further information has been made publicly available.
Cuba’s vaccine COVID coverage is among the best in the world.Yander Zamora/EPA-EFE
Around 90% of Cuba’s 11 million people have received at least one dose of a COVID vaccine, with 82% considered fully vaccinated, and it appears
Cuba is vaccinating children as young as two. Both Abdala and Soberana
have been used, with around 8 million people receiving three doses of
Abdala.
Following a big spike in cases
in August 2021 – when the country’s vaccine coverage was still
relatively low – new infections in Cuba have since declined greatly and
remain low. Without proper studies, it’s difficult to gauge how much of
this is down to the vaccines, but the virus’s suppression coinciding
with the country reaching high vaccine coverage is a positive sign.
Who could use a Cuban vaccine?
Given the difficult relationship between Cuba and the US, the market
for Cuba’s vaccines will probably be its political allies. Vietnam and
Venezuela are reported
to have received Abdala doses, Nicaragua has given emergency
authorisation to both vaccines, and doses have previously been sent to Iran for use in clinical trials. Mexico and Argentina are also interested in using these vaccines.
Cuba has submitted both to the World Health Organization (WHO) for
approval, which would improve the likelihood of them being used abroad.
If there are any plans to include them in the Covax vaccine-sharing
initiative, then WHO approval is a must.
Meanwhile, we’re still waiting to see what impact omicron will have. So long as there’s unequal access to vaccines, the pandemic will continue – and so too the risk of new variants arising.
Given most richer countries aren’t in the queue for Abdala or
Soberana 02, it’s entirely possible that in future, parts of South
America, Asia and Africa – where vaccine coverage is particularly low – may see Cuban vaccines in many arms.
From
his home in Portola Valley, California, Sanjiv Gambhir logged on to an
important meeting for his startup one afternoon in April 2020. He kept
the video camera off.
advertisement
This
was unusual, not least because he cherished face-to-face connections
and was obsessed with visibility. A pioneer of molecular imaging and the
director of Stanford’s Canary Center for Early Cancer Detection,
Gambhir, known as Sam, had spent decades trying to make small, hidden
tumors inside the body easier to see. Nearly 600,000 people in the U.S.
die from cancer every year, mostly because we tend to catch tumors when
they’re too late to effectively treat.
“Cancer doesn’t need to be a
death sentence,” Gambhir would tell the researchers in his lab, as he
reminded them of the actual patients they were trying to save. By the
time he was 50, his breakthroughs in early detection—including
developing the reporter genes used in positron emission tomography, or
PET scans—had led to three startups, millions in seed funding, and 40
patents.
His latest startup, Earli,
was the culmination of a decade’s-worth of research into whether you
could force tumors to show themselves, by having them send out a signal
that could be detected in blood tests or PET scans. If that worked, you
could open up a new frontier in cancer detection. Gambhir had pioneered
the technology, but cofounder Cyriac Roeding, an energetic e-commerce
entrepreneur had convinced him to turn it into a company. By the start
of 2020, they had already raised $19.5 million in venture funding to
fuel the commercialization of their technology.
advertisement
But
in 2019, doctors had detected something inside Gambhir. A tumor of
unknown origin was quietly spreading in his bones. The irony of cancer
sneaking up on him was as brutal as the prognosis: After finding such
metastasis, the median survival time is three to four months. But
Gambhir turned his cancer and his experimental treatments—every few
weeks in Munich—into a learning opportunity for himself and his
colleagues. Now, a year after his diagnosis, he was bedridden and weak
from the treatments. But he was determined to be on this call.
For
three hours, Gambhir and the rest of the five-person board—including
Jorge Conde, a biotech veteran and partner at the prominent venture
capital firm Andreessen Horowitz—discussed manufacturing challenges, the
search for more cash, and the results of a recent study the company had
done in mice. “He was sharp as a tack. I mean, for God’s sake, the guy
was still pulling apart the science,” says Earli cofounder and chief
scientific officer David Suhy. “But you could hear in his voice, he was
physically weak.”
Sanjiv Gambhir [Photo: courtesy of Earli]Gambhir
was often reminding his cofounders how bedeviling biology could be, how
resistant it was to commercialization. “The world of biology will
always find a way to screw you over,” he’d warned Roeding as they were
founding the company in 2018. After establishing Stanford’s
Multimodality Molecular Imaging Lab in 2003, Gambhir had helped develop
an armory of futuristic advances for spotting tumors, including a smart
bra to continuously monitor for breast cancer and a smart toilet for
detecting colon cancers. But much of the tech was still experimental.
advertisement
As
Gambhir pursued this research, his wife, Aruna, battled back breast
cancer—twice. Then, in 2013, biology reared its head in another,
horrible way: Their 15-year-old son, Milan, was diagnosed with a rare
form of the most aggressive kind of brain cancer, the very type of tumor
Gambhir’s lab had been studying. Gambhir’s need to translate his work
from lab to practice had never been more urgent. But Milan’s cancer
proved quicker than the pace of medicine. He died in 2015, at the age of
16.
Five years later, as a tumor spread in his own body, Gambhir
felt a different kind of urgency. “The problem is, he knew too much,
even with Milan,” says Aruna. Now Gambhir’s ideas and multi-disciplinary
insights into molecular imaging—his one-of-a-kind knowledge of the
field—would need to go to the scientists and doctors who could make the
most of it, even in his absence.
When President Nixon launched the
war on cancer 50 years ago, Sidney Farber, the president of the
American Cancer Society, declared that with enough resources, scientists
could conquer cancer in seven years. Instead it has been a protracted
war with a roving target. Despite hundreds of billions of dollars spent
on research, cancer is now vying with heart disease to be the number one
cause of death in the U.S. “Since 1970, there’s maybe 50% improvement
in cancer survivors,” says Leland Hartwell, an advisor to Earli whose
work on cell growth earned him a Nobel Prize in Biology. “Given all the
effort, it’s not great.”
advertisement
The
hope now isn’t a cure, but finding the right combination of diagnostics
and treatments to manage it. And after years of relatively miniscule
government funding, detection is getting more attention. The race to
catch cancer earlier has given rise to a $168 billion industry
touting a new class of tests that promise to detect tiny signs of
cancers in your blood or stool. Most are pursuing an approach known as
“liquid biopsy,” using a blood test to look for abnormal pieces of DNA
shed by cancer cells.
Finding bits of cancer cell sheddings,
however, is notoriously hard. Earli’s approach compels tiny tumors to
produce new signals, sending out flares—naturally-occurring
proteins—that can be more easily detected in a blood test or illuminated
for an imaging scan. A reliable diagnostic that could be administered
once a year by a doctor to find and pinpoint very early, aggressive
tumors in apparently healthy people could have a profound impact on
healthcare and its costs.
“Once you find [a tumor] and you can
localize it, you can act on it, and then it becomes protection, not just
detection,” Roeding says. Someday, Earli’s “synthetic biopsy” platform
could even be useful for targeting cancer cells with personalized
medicine, immunotherapies, or mRNA vaccines. Already the company has
shown an ability to detect certain cancers in mice and dogs; in June, it
began dosing its first human patients as part of a clinical trial. But
it still has a long way to go.
advertisement
Back
at the board meeting, Roeding reviewed the results of their first trial
in mice. The synthetic biomarker they were using to tag tumor cells had
shown up in PET scans of cancerous mice—a little glowing lighthouse in a
sea of uncertainty. Suhy and Roeding were ecstatic. Gambhir was
circumspect. “He asked us four questions,” Roeding recalls. Did the test
actually detect cancer? Did it have a low false negative rate? Was it
differentiating between malignant and benign? Could it determine the
stage of cancer?
The trial was promising, but Gambhir needed more
than promises. In June 2020, three months after the board meeting—and
the day after receiving Stanford’s Dean’s Medal, its highest honor—he
died at home at the age of 57.
For
the field of early cancer detection, the loss was devastating. Tributes
poured in from researchers around the world, and colleagues held a
string of academic symposia dedicated to his legacy. Last September, the
Journal of Nuclear Medicine bucked a 55-year tradition for the cover, trading its typical medical imagery for a full-page portrait of Gambhir.
advertisement
His
company, meanwhile, is forging ahead and confronting another big
question: Can they manifest a technology without the visionary who
dreamt it up? “We are working on a very low probability, but potentially
high impact thing,” says Roeding. “It’s a moonshot. There’s no doubt
about it.”
Light-haired and boyish, Roeding was born in
Germany, and yet is the archetypical energetic Silicon Valley
entrepreneur-investor. A veteran of business consulting, smartphone-era
startups, and venture capital, he can repeat a well-rehearsed pitch
verbatim and never sound scripted—skills that helped him build up the
in-store discount app Shopkick and sell it for $250 million to the
biggest telecom company in South Korea.
In 2016, a couple years
after that deal, Roeding was in the Bay Area looking for his next
startup idea. An interest in brain-computer interfaces brought him to
Stanford’s campus, which in turn led him down the rabbit hole of
precision medicine. But the deeper he got, the more confused he became.
Here were all these scientists saying they each had the solution to the
world’s various biggest problems. “I’m not a biologist,” says Roeding.
“I didn’t know who was wrong.”
advertisement
By
Thanksgiving, three months into his search, Roeding was feeling
deflated. That morning, his wife handed him a copy of Stanford’s alumni
magazine and suggested he read the cover story, about a prominent
radiologist’s struggle to save his son from metastatic brain cancer. The
piece shook him, and early that afternoon he sent an email to its
subject, Gambhir. “I can only imagine how hard especially holidays like
today’s are for you and your wife,” Roeding wrote. “But perhaps just on a
day like this, it is worth remembering that Milan, your journey to try
to save him, and the powerful ideas that have come from this journey,
have inspired others like me.” Roeding introduced himself, and said he,
too, was interested in health monitoring. “Perhaps there are ways we
could work together.”
Two months later, they met on a sun-drenched
Saturday at a small restaurant in Portola Valley, a town near Palo
Alto. They talked about innovation and science and the yawning chasm
between academia and commercial medicine. After years of navigating the
bureaucracies of biomedical research, Gambhir was drawn to Roeding’s
left-field thinking. The lunch became the first of many Saturday
meetings. Gambhir agreed to teach Roeding biology (“largely in vain,”
says Roeding) and introduced him to even more scientists. But Roeding
was more eager to hear what Gambhir was working on. When Gambhir told
him about his lab’s work around using biomarkers to catch tumors earlier
than other diagnostics, Roeding was hooked.
They used $400,000 of
their own money to get started, incorporating the company in June 2018.
They negotiated a licensing deal with Stanford for Gambhir’s related
patents and tapped Suhy, who previously led gene therapies at Australian
biopharma Benitec, to serve as chief scientific officer. Gambhir would
be a scientific advisor and Roeding became CEO.
advertisement
Earli cofounders Cyriac Roeding, Sanjiv Gambhir, and David Suhy [Photo: courtesy of Earli]Roeding
was an unusual choice to helm a breakthrough biotech company. He
recalls asking Gambhir: “Should someone with my background bother the
world of biology with my presence?” The field of biology has a surplus
of experts and no generalists, said Gambhir, and few people who knew how
to run a startup. On top of that, he said, biology is fickle:
biological exploration will always take longer and be harder than you
think. He argued that being able to move fast—and, yes, fail fast—could
help the company resist the inertia of experiments, trials, and
regulations.
At the start, Roeding’s aggressive targets raised
eyebrows among investors. “We said, we want to be in humans within three
years, and they kind of chuckled,” says Roeding. Most weren’t
convinced, but the pitch caught the attention of Andreessen Horowitz’s
Conde, who is a biotech industry veteran. Before the year was out,
Gambhir and Roeding had secured just shy of $19.5 million in seed
funding from a group led by Andreessen Horowitz that included Salesforce
founder Marc Benioff, Menlo Ventures, and Chinese venture firm
ZhenFund.
Even with buy-in from the likes of Andreessen and
Benioff, the founders knew their operation faced an uphill battle.
Diagnostics that require injecting patients face a phalanx of clinical
trials, a process that takes years even with the enormous resources of
giant pharmaceutical companies. While Earli had shown some promise in
the lab, there wasn’t a guarantee it would translate to animals. And
scientists had never tested synthetic biomarkers in humans: There were
likely to be unusual regulatory hurdles to getting a clinical trial
approved.
advertisement
For
the first year, Suhy and Roeding met with Gambhir every four to six
weeks to talk about the company’s progress. They managed day-to-day
operations, but Gambhir could find the holes in their thinking and minor
successes—an invaluable perspective in setting the direction until
their next meeting. As the hours wore on, their conversations would
inevitably give way to heady discussions on the state of science.
In
late spring of 2019, Roeding got a call from Gambhir. His voice sounded
funny. He told Roeding that he was sitting on the couch with his wife.
They had just found out that he had cancer, and it wasn’t clear where it
had started. By definition, it was metastatic and almost impossible to
treat. If they didn’t know where it originated, they couldn’t know what
they were fighting.
Roeding tried to stay optimistic. “It’s battle
time,” he told his cofounder. Gambhir said there were possible
treatments, but he was also clear-eyed. They agreed that they needed to
prepare the company for a world without Gambhir.
advertisement
“We
have to make sure that our science is advanced enough so that we can
move forward without having to rely on his input at a deep level
continuously,” Roeding recalls realizing. “For us, really the main
question became, does Earli have enough escape velocity so that we can
become what [Gambhir] wants us to be?”
The biggest victories
in the war on cancer have been scored via anti-smoking campaigns and
cigarette taxation. They’re largely responsible for the 27% drop in
deaths from cancer in the U.S. between 2009 and 2019, according to the
Center for Disease Control and Prevention (in lung cancer, advances in
targeted therapies also played a role). Still, little has progressed in
screening, which scientists see as the best opportunity to find cancer
before it gets out of control.
Chances are, you’ve been through
multiple cancer screenings: mammograms, pap smears, colonoscopies, when a
doctor takes a look at the weird mole on your back. Long-time smokers
over 50 years old might get a CT scan. For certain cancer types, these
screens, which mostly rely on seeing physical changes, can save lives.
advertisement
But
there are lots of forms of cancers that can’t be screened for: ones
that are too small to see or that haven’t necessarily caused any bodily
changes. Tumors mutate and evolve in unique ways, so each person’s
cancer is a little different. A tumor that’s benign in one body could be
deadly in another. “What we’re faced with is just enormous diversity,”
says Earli advisor Hartwell.
As a result, cancer treatment has
become more personalized, with scientists tailoring dosage and type of
therapeutic to the genetic makeup of a cancer’s cells. But some
scientists, including Hartwell, think that developing better earlier
detection methods will offer a far less invasive—and far more
affordable—path to lowering cancer deaths. So far, however, early
detection has proceeded in fits and starts. “The cost per advance is not
impressive,” he says.
[Photo: courtesy of Earli]The
latest and greatest tools in cancer diagnostics are genetic testing and
liquid biopsy tests. Genetic testing alerts doctors to potential genes
that are associated with an increased risk of cancer, like BRCA-1 and
BRCA-2 for breast cancer. Liquid biopsies capitalize on advances in
machine learning to analyze blood samples for the tiniest clues of
cancer, by detecting and analyzing fleeting fragments of cells that
tumors shed. These can include DNA, RNA, proteins, and other pieces of
cancer cells that circulate in the body and sometimes contain clues
about their location.
advertisement
Menlo
Park-based Grail—one of dozens of companies that Gambhir advised—now
sells a liquid biopsy test called Galleri, which purports to find 50
types of cancers in apparently healthy people. The test, at $950, is not
covered by insurance, but that could change after full FDA approval,
which Grail intends to seek in 2023. Another California company,
Redwood-based Guardant Health, is currently running trials of its
early-stage colorectal cancer test, eyeing a market for early detection
that’s expected to reach $280 billion by 2027.
Not everyone is so
bullish on liquid biopsies, however. “I should be careful what I say. I
could make myself persona non grata,” says Judy Garber, Director of the
Center for Cancer Genetics and Prevention at Dana-Farber Cancer
Institute and board member to Earli. Several liquid biopsy companies,
she says, “want to find all cancer at once, which I agree would be
great. But I think that hasn’t been what the data supports, and yet they
seem to be in this huge rush to sell their test.”
The most compelling recent data
showed that Grail’s test could positively identify stage I to III
cancer more than 67% of the time in a set of twelve cancers including
head and neck, liver, and pancreatic cases. Overall, the test had a
false positive rate of 0.5%, and was able to identify the tumors’ organ
sites 88.7% of the time. But its ability to detect other cancers was
lower: It identified less than 20% of thyroid, kidney, and prostate
cancer cases, for instance.
[Photo: courtesy of Earli]One
major challenge with looking for natural biomarkers, like cell
sheddings, is that young tumors produce far fewer of these fragments.
Even when these cancer bits do make it into the bloodstream, they spend
less time in circulation, making it exceedingly difficult to pull them
out in a sample.
Earli’s diagnostic takes a more proactive
approach to the search for tumors. The platform consists of an
injectible compound that carries a reporter gene, engineered to activate
at the faintest hints of tumor cells, wherever they are. Once it’s
tapped into the cellular pathways driving the tumor’s uncontrolled
growth, the gene is designed to express a synthetic biomarker,
effectively “boosting” the cancer’s signal. For its biomarker, Earli
chose an enzyme that typically only appears during embryonic
development. (A Cambridge-based startup called Glympse is developing
synthetic biomarkers to identify liver disease, though cancer detection
is also on its roadmap.)
The approach has several apparent
advantages over current liquid biopsy technologies. Because it uses a
synthetic biomarker, Earli can more easily control the amplitude of the
signal. Where liquid biopsy companies use the genetic code of cancer
fragments to try to determine a tumor’s location in the body, Earli
pinpoints the tumor itself. This could also help physicians better track
the success of ongoing therapies, and lead to novel therapies: With an
additional molecule designed to trigger an immune response in cancer cells, Earli’s surveillance platform could eventually be harnessed to kill elusive tumors too.
Hartwell
remembers hearing Earli’s concept for the first time, and being struck
by it as “incredibly brilliant.” “You sort of wonder why it took us so
long to think of it,” he says. “But that’s not what makes a successful
company.” If Earli is going to be “a company rather than just a research
project,” he stresses, it needs to quickly identify—and market—an
application of its technology. “That’s a race that you can’t predict.”
When
Gambhir died, the company was still in semi-stealth. Earli barely had a
web presence, save for a recruiting website, and had interesting, but
nascent progress in mice. It needed more cash, to hire more scientists,
double down on pre-clinical research, and start building out a new lab.
Before
Gambhir’s last board meeting, the company began getting feedback from
his longtime colleagues and friends, a Who’s Who of cancer pioneers:
Hartwell and Garber, but also Nobel Prize-winning cancer researcher Jim
Allison, Moderna founder Bob Langer, Charlie Rudin, who heads up
thoracic oncology at Memorial Sloan Kettering, and Aruna, who now runs
another company related to her husband’s research called CellSight,
which is working on technology that recognizes if cancer treatment is
working.
In fall 2019, Langer dashed off an email to investor
Vinod Khosla, founder of Khosla Ventures, introducing him to Earli and
laying out how it differed from liquid biopsy firms. Khosla had for
years passed on high-flying biotech investments, but says he was drawn
to Earli’s “orthogonal approach” to early detection, versus the
“incremental” efforts of other ventures. Khosla likens Earli to
Cambridge-based Commonwealth Fusion Systems, one of his biggest
investments, which is aiming for the moonshot of nuclear fusion. “In our
fund, we sort of say, ‘large impact, large technology breakthroughs
that cause a large impact’—if you do that, the money will follow.”
Dr. Michael Kent, pictured with his dog Danson, is helping Earli conduct trials at his canine lab at UC Davis [Photo by Don Preisler/UCDavis]In
January 2020, Khosla Ventures led Earli’s $40 million series A,
alongside Andreessen Horowitz. The board now includes Conde, Justin Kao,
who led Khosla’s investment, and Marc Andreessen, who serves as a board
observer.
“It’ll never be quite as good as if Sam was working
on it himself,” Khosla admits, “but they’re at a proof point that is
substantially lower risk today than it was two years ago.” He pointed to
“a cadre of world-class scientists” that Earli has recruited as
advisers. “If it can be done, I think this team can do it.”
With
the funds, Earli went on a hiring spree: 29 researchers now work at its
headquarters in South San Francisco. And Roeding and Suhy decided to
pursue a proof of concept in dogs. The company worked with the
Comparative Cancer Center at the University of California Davis School
of Veterinary Medicine, which connects sick dogs with clinical trials.
Together they studied the biomarker at four different doses in a total
of 23 dogs to see if it would show up in blood work.
Roeding and members of the Earli research team [Photo: courtesy of Earli]Michael
Kent, director of the center, says that Earli’s compound was well
tolerated, with only a few dogs developing a brief and low-grade fever.
Full trial results of the trial will be published later this year, but
the results were favorable. “This isn’t going to be in your doctor’s
office next year, but this could be game-changing,” Kent says. Unlike
the liquid biopsy tech Kent has tested, Earli doesn’t depend upon
serendipity to spot cancer. “You have something making a clear signal
and saying, ‘Hey, I’m here!” That’s unique.” Earli is now funding
subsequent trials with dozens of dogs.
Demonstrating that the
test was nontoxic for dogs was crucial in getting the Australian
government to agree to let Earli begin its first human trials in the
country, which began this past September. So far, two people have been
dosed, and another is on track. The aim is to detect advanced-stage lung
cancer in already diagnosed patients—and to amass the data Earli will
need to convince the U.S. Food and Drug Administration to let it proceed
with a U.S. trial of its novel technology.
Suhy says he’s
encouraged by the speed with which the FDA approved mRNA vaccines during
the pandemic. That suggests regulators are amenable to novel medical
technology like Earli’s diagnostic. Still, he notes, those approvals
were based on years of data. And even if Earli achieves FDA approval, it
will need to convince doctors to add a novel diagnostic to their
workflow.
Nora Pashayan, a professor of Applied Cancer Research at
University College London who is not affiliated with Earli, calls its
concept “amazing.” But says “it could take a long time” for Earli to
come to market. And its approach faces several pressing questions, she
says, related to the design of the biomarker, how often it’s deployed,
and in whom.
These elements—how and who—matter, because contrary
to conventional medical wisdom, early detection doesn’t always save
lives. The problem is that doctors can’t always tell the difference
between a benign or malignant tumor and therefore may treat a tumor out
of an abundance of caution. “Other than the psychological burden [of
diagnosis], there are side effects of treatment—going into chemotherapy,
endotherapy, or surgery,” says Pashayan. “So the harms are much more
than the benefits, [if] this cancer was not going to do anything.”
A failed public health effort in South Korea serves as a cautionary tale.
Between 2000 and 2011, thanks to a government recommendation, doctors
in the country started screening everyone for thyroid cancer.
Unsurprisingly there was a surge in thyroid cancer diagnoses and surgery
to remove these tumors. However, after ten years, deaths from thyroid
cancer remained stable. The screening campaign wasn’t preventing death.
If anything, it was creating problems for people who were experiencing
complications from unnecessary surgery. For companies like Earli, the
protocols around a diagnostic matter as much as whether it works.
The
greater scientific research community still believes that early
detection tools, like Earli’s, are critical. Cancer drugs treat, but do
not cure—and are immensely expensive. The hope is that finding cancer
early, identifying the tumor profile, and stopping it before it spreads
could one day make getting cancer a relatively anxiety-free experience.
“What we need to show are the success cases of what it means to find it,
get rid of it, and live on,” says Roeding. “And in order to do that, we
need to find more early stage cancers.”
More than 1,600
people logged into Gambhir’s memorial service, which was held at the
height of the pandemic, in July 2020. Colleagues described his
generosity and far-sightedness. “It would not be entirely accurate to
say that Sam presented a ‘vision’ for the field of molecular imaging,
because that sounds a little like the elements of the vision were out
there and others were also aware of it,” said Norbert Pelc, Stanford
University professor emeritus of radiology. “Sam created the vision and
then articulated it. He was able to do that: See a path ahead many years
ahead of his time and explain it to an audience at a wide range of
levels.”
“He gave you confidence in that future,” says Christina
Zavaleta, an assistant professor of biomedical engineering at USC and
one of Gambhir’s hundreds of former students. Sam may not get to see
where all of his ideas will travel, but “he was already there in his
mind,” she says. “We’re the ones that have to catch up.”
[Photo: courtesy of Earli]
Gambhir’s
technology is bound to introduce new conundrums, about if and how to
treat previously hidden tumors. Even if Roeding and Suhy can
successfully render Gambhir’s novel early detection technology into a
marketable diagnostic, it won’t end our battle with cancer. Still, if
they can pull it off, it could give patients and doctors the luxury of
choice, something that Sam and Milan Gambhir didn’t have.
“It’s
a cruel irony that Sam’s own cancer was only detected after it had
spread to his bones,” Aruna, Sam’s wife, said at his memorial, her voice
breaking. “Perhaps if some of the tools in precision health were in
place, he would have had a chance to live and contribute even more. He
told me towards the end days that he felt he had another decade of
productive work left in him. Imagine what that could have meant for
humanity.”
")



 Saikia in intensive care: the transplant has led to questions of medical ethics
Saikia in intensive care: the transplant has led to questions of medical ethics
















 [Photo: courtesy of Earli]
[Photo: courtesy of Earli]